social development
Post-1995 health policies
In 1995, the enactment of the National Health Promotion Act marked adramatic shift in long-term health care planning from a focus on treating serious diseases to one on preventing diseases and promoting a healthy lifestyle. The reason for the shift was a change in disease patterns. While a cute infectious diseases declined dramatically in the 1970s and 1980s because of increased vaccine supplies and improved sanitation, chronic diseases such as hypertension, diabetes and cancers multiplied due to lifestyle changes, an aging population and deteriorating environmental conditions.
The government started the National Health Promotion Fund in July 1997, which was financed by a 2 won tax per pack of cigarettes. In 1998, the Ministry of Health and Welfare set up a department to implement health promotion programs such as hypertension control. The number of key health promotion centers increased from nine to 19 between 1998 and 1999 and the “Korea Health Fair” was held in 2000. The National Health Promotion Plan 2010 was launched in 2002, with the goal of achieving improvements in physical and mental health by 2010, including raising the disability-adjusted life expectancy from 66 years in 2002 to 75 years in 2010. The health promotion tax was raised to 354 won per pack of cigarettes in 2004, which supported activities at all of the 246 health promotion centers nationwide.
The government also introduced asignificant change in the organization of the NHI system to improve managerial efficiency and address the financial instability of the community-based health insurance scheme. 32 The latter was merged with the scheme for civil servants and private school employees 1) in October 1998, and then with the company based insurance scheme 2) in July 2000. At first, the mergers led only to the consolidation of administrative organizations of the different schemes. The full consolidation of their financial systems followed three years later and the cross-subsidization between the different groups of participants began in earnest. The National Health Insurance Corporation (NHIC) is now in charge of administering the entire NHI system as the single insurer of the public health insurance scheme.
Questions remain whether the consolidation produced promised efficiency gains and promoted fairness in the burden of contribution among participants. The number of the NHIC regional offices fell by one-third after the consolidation as did the number of its total employees, 3) but the lack of consumer choice and competition between insurers in the single-insurer system can reduce NHIC’s incentive to improve efficiency further. The impact of cross-subsidization on the fairness is more difficult to assess because data on the income of the self-employed and other community-based participants is far less complete than that of company-based participants.
In 2000, there was a dramatic reform that separated the functions of doctors and pharmacists in terms of dispensing medicine. Doctors could no longer dispense drugs directly to patients, who now had to buy them from pharmacists. At the same time, pharmacists could no longer sell antibiotics and other types of medicine to consumers without adoctor’s prescription. Additionally, the NHI system separated reimbursements for pharmaceuticals from medical care.
The new system was meant to crack down on the over-prescription of medicine as well as to curb the abuse of drugs. Other objectives included encouraging the specialization of medical and pharmacy practices, promoting the early diagnosis of diseases by requiring patients to visit doctors instead of relying on the advice of pharmacists, and improving the patients’ right to know. The system was slated to come into effect in August 2000, but the government, doctors and pharmacists reached full agreement on its implementation only in November after both doctors and pharmacists shut down their operations in protest at the new measures.
The system continues to remain controversial. Medical cost rose sharply since then, 4) and there is no clear sign that the abuse of drugs has been curbed. Still, the reform is generally accepted as irrevocable and astep in the right direction.
Another challenge that the government had to deal with was the mounting NHI deficit that began in the mid-1990s. Until then, the NHI system had been financially stable, with reserves of 4 trillion won at the end of 1995. But it suddenly recorded deficits from 1996, asituation made worse by the 1997 financial crisis.
Several major reasons have been citied for the growing deficits. One was that increases in the NHI premiums were not large enough to keep up with the increase in health care expenditures caused by an increased use of medical services, an aging population and arise in the number of expensive medical treatment. In addition, the policy of separating the functions of doctors and pharmacists created adeficit of 1.9 trillion won in the NHI system by 2002, which exhausted its accumulated reserves and forced the government to resort to short-term borrowing to fill the gap. In response, the government enacted the Special Act to Stabilize National Health Insurance Finances in January 2002, which required the government to finance afixed portion of NHI spending from the general tax revenue.
At the same time, however, the government boosted spending growth. A target for the benefits coverage ratio was established to ease the burden of out-of-pocket expenditures by patients (August 2005). The out-of-pocket ratio for seriously ill patients, such as cancer patients, was lowered to 10 percent (September 2005), the meal costs of hospitalized patients came under benefits coverage (January 2006), the out-of-pocket payment for hospitalized children under 6 years of age was exempted, and similar benefits began to be provided for medicines used to treat rare or catastrophic diseases. As a result, the NHI benefits ratio reached 64 percent in 2006, with the benefits ratio for cancer patients increasing from 50 percent in 2004 to 66 percent in 2005.
In the mid-2000s, the government focused on expanding the public health care system.
Various initiatives 5) were formulated and incorporated in acomprehensive plan for promoting public health care. The plan included developing community-based hospitals, strengthening cancer programs at the national level, and reinforcing measures to tackle infectious diseases, with abudget of 4.3 trillion won appropriated from 2005 to 2009. In addition, 235.9 billion won in special taxes targeted for rural area development was used to improve the medical facilities at public health centers in rural areas.
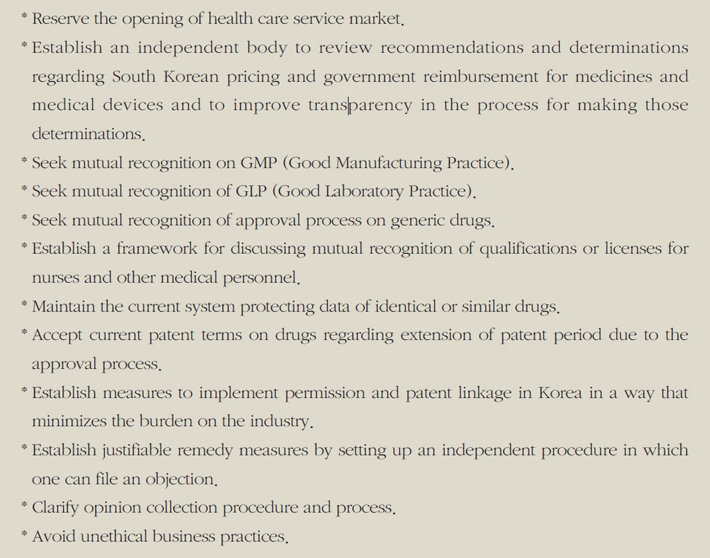
In the meantime, a free trade agreement between Korea and the United States (KOR US FTA) was finally concluded on April 2, 2007 after 14 months of negotiations. A major issue for negotiations concerning health care was the further opening of the Korean market to U.S. pharmaceutical products. The opening of health care service market was reserved for future negotiation (Table 6-14).
Table 6-14. Agreements of the KORUS FTA in the health care sector (December 2008)
Another significant change was the partial opening of the health care service market.
The Act on the Designation and Operation of Free Economic Zones was revised on January 27, 2005 to allow foreign medical institutions to treat local citizens within the free economic zones. Additionally, the Special Act on the Establishment of Jeju Special Self-Governing Province and the Development of Free International Cities was promulgated on February 21, 2006 to allow foreign medical institutions to be established on the island of Jeju. Although these measures have not resulted in the establishment of a single foreign-owned hospital in these areas, it is seen as amajor step in terms of establishing the principle for the further opening of the medical services sector later.
Source : SaKong, Il and Koh, Youngsun, 2010. The Korean Economy Six Decades of Growth and Development. Seoul: Korea Development Institute.
NOTE
1)This had been administered through the Insurance Society for Government and Private School Employees.
2)The company-based scheme had been administered through the Insurance Societies for Employees. There existed 140 such societies at the time of merger
3) The number of regional offices fell from 385 to 241 and the number of employees from 15,653 to 10,454 (Sang Seok Lee, 2003).
4) Possible reasons for the sharp rise include the addition of pharmacist’s dispensing fees to the cost of drugs and the increased prescription of expensive drugs by doctors who now have no incentive to prescribe less expensive drugs
5) Health Plan 2010 (2005), Combat Cancer 2015 (2006), Strategy for Executing Health Investment (2007), Public Health Care Expansion Plan (2005), Basic Plan for Emergency Care 2005-2010 (2005), Government Plan for Health Care Development (2003), Basic Plan for Health Care Personnel (2006), 2010 Health Care Industry Development Plan (2006), Korean Traditional Medicine Development Plan (2005), and others.
References
· Lee, Sang Seok,“ The Financial Consolidation of the National Health Insurance System: Its Necessity and Future Plans,”Bok Ji Dong Hyang, May 2003, (in Korean).